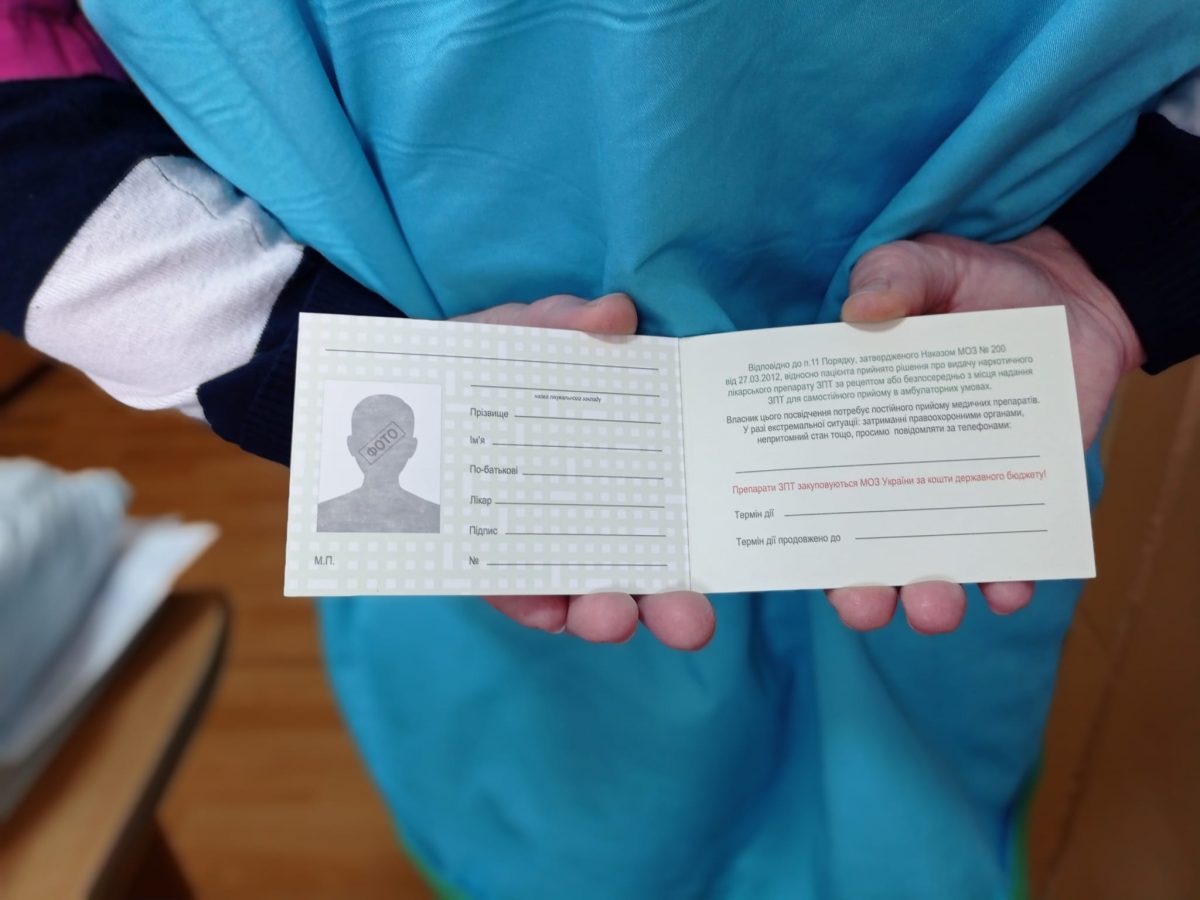
In 2021, the REAct system recorded 22% of cases of violations of OST patients’ rights. Violations usually concerned illegal searches and police detention of clients who had OST medications for self-reception. Although OST patients usually have documents proving the legality of obtaining the necessary drugs with them, this information is often insufficient for police officers. In such cases, they can call the medical facility to find out if the person is really a patient of the Program, or forcibly take him to the police station to further determine the reasons for the person’s drug findings. To reduce the reasons for such situations between OST patients and police officers, the REAct project team initiated the widespread introduction of an appropriate advocacy mechanism. Currently, our colleagues from ICF “Alliance for Public Health” are actively lobbying for amendments to the legal act governing the implementation of the OST program – Order of the Ministry of Health of Ukraine from 27.03.2012 № 200 “On approval of the Procedure for substitution maintenance therapy for people with mental and behavioral disorders due to opioid use”, to provide OST patients with appropriate certificates of program participants. As a result of such work, a pilot phase was agreed upon by the relevant group at the Ministry of Health in February this year. As of May 2022, partners of the ICF “Alliance for Public Health” have already begun to receive forms of “OST Patient Certificate” for further issuance to interested patients who receive drugs for self-reception for up to 30 days. The forms also include the OST Patient’s Note, which contains an algorithm for the patient’s actions in various situations. Those wishing to obtain a certain number of copies of the OST Patient Certificate should fill out the form at: https://forms.gle/an1ybF1PZeYe6bUe8. We remind you that we are currently collecting real needs to decide on the next edition. The deadline for applications is May 15, 2022.
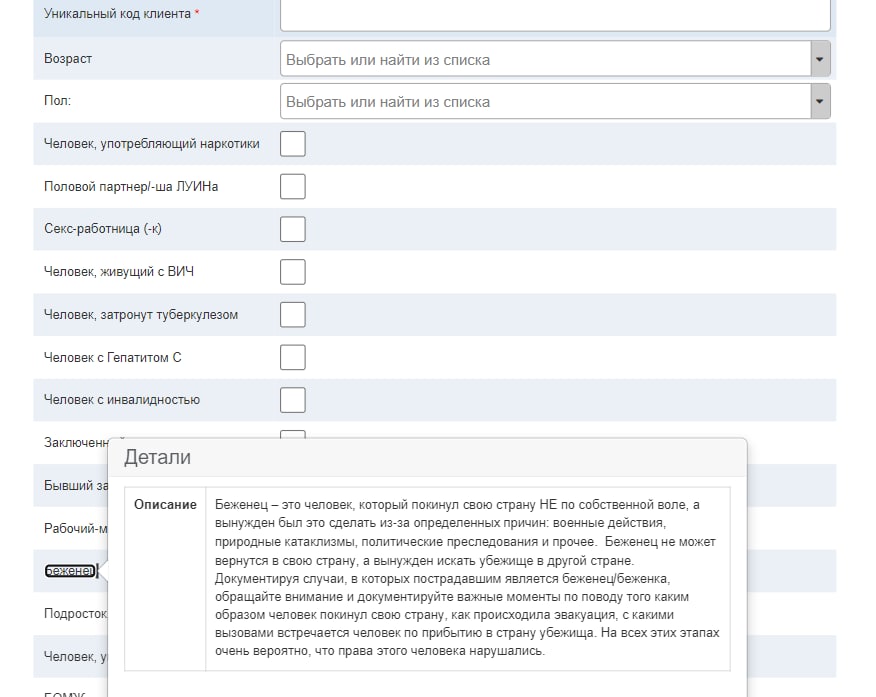
The full-scale war on the part of the Russian Federation (RF) in Ukraine on February 24, 2022, significantly affected the implementation of the REAct system. In particular, it affected the work of documentaries in the regions, mechanisms of interaction with clients, customer needs, and the implementation of the appropriate response. An additional category of people has emerged in the REAct system as a risk group assisted by the Project – refugees, which include both internally displaced persons (IDPs) and those who have been forced to move abroad.
Prior to the armed aggression, the REAct project operated in 18 regions of the country. However, so far some of the documentaries from the most dangerous regions have had to travel to other cities in Ukraine or abroad. Among them are most documentaries and coordinators of Mykolaiv, Kharkiv, Kyiv, Chernihiv, and Zaporizhia regions. Some continue to stay in Ukraine and serve in the Armed Forces of Ukraine or the Territorial Defense, some volunteer, help internally displaced persons, and accompany humanitarian aid.
Kharkiv. Photo: Alex Lourie
Currently, most clients’ inquiries concern the inability to receive vital treatment in time, or obstacles to obtaining it at a new location (SMT, ART, anti-TB drugs), issues of recovery/conclusion of declarations with a family doctor, difficulties in obtaining temporary housing, the need for an evacuation from the hottest spots, barriers to receiving other services against the background of temporary job loss.
Interaction with clients is mostly online and by phone, but the working hours of documentaries have increased during the day. In urgent cases of clients and due to the limitations of martial law, in some cases, there is also direct support for the client in resolving his case. Documentaries point out some circumstances that sometimes complicate or prolong the process of resolving clients’ cases. Among them: reduced time for receiving specialists in social services and hospitals, temporary cessation of services to individual specialists and institutions, and re-profiling the activities of partner organizations.
Starting from March 3, 2022, Kherson is under blockade by Russian troops with all the logical consequences: lack of supply of food and medicine, the danger of movement in the city, inability to move around the region, power outages, and Internet communications. Currently, all work of REAct documentaries in this area is carried out exclusively remotely. Among the services provided: are psychological support, initial legal advice, and social support. Due to the remote format of the work, it is currently not possible to provide assistance to applicants in cases of humanitarian need, namely food or essential medicines.
“Due to frequent shelling and poor quality or sometimes no communication at all, it is not always possible to provide assistance and therefore the applicant’s situation may worsen”, – said Kutsenko Volodymyr, coordinator in the Kherson region.
At the level of Kherson oblast, the work of representatives of state institutions with key groups is completely absent due to the occupation and blockade of settlements in the region. However, in the city, the work continues in an active and effective format.
The number of appeals from citizens has increased significantly since the beginning of the war in the Kherson region. This applies to all categories of the population without exception. Appeals are usually made on issues such as the need for food; the need to purchase drugs, undergo treatment; psychological support; social benefits; the possibility of evacuation; compensation for damage caused in connection with the start of full-scale hostilities, and armed aggression directly in the Kherson region.
Currently, due to a lack of communication, it is not possible to obtain information on the status of the Project in Chernihiv. However, it is known that a number of documentaries left the city and went abroad.
In the Kyiv region, the work was adapted to the real conditions of the war. Clients turn to documentaries by phone or messenger. Cases of violation of rights are resolved through consultations, referral of clients to friendly specialists, and sending appropriate letters to government agencies.
“It is difficult to work in these conditions because the laws of war are in force. In some cases, human rights are restricted, as is the order in which cases of violations of rights are resolved, as priority is given to violations of the customs of war. Therefore, some cases that need to be resolved at the state level have been postponed until better times”, – said Ivan Viktorov, coordinator in Kyiv region.
Kyiv. Photo: Sergey Korovayny
Due to the occupation and blockade of Melitopol by Russian troops and the difficult situation in Zaporizhia, interaction with customers in these cities is also remote. Many appeals are received regarding access to ART, anti-tuberculosis treatment, SMT. However, representatives of public organizations try to meet the needs of clients in treatment by delivering drugs to patients and transporting patients to appropriate medical facilities. We also managed to establish cooperation with volunteers, through whom humanitarian aid is received and provided to Project clients.
In Odesa Oblast, documentaries noted that the war did not critically affect the Project work. NGOs continue to operate, with most social workers on site. Work in the Odessa region, as in other regions, is carried out mainly by telephone, calls are now received throughout the day and night. Personal meetings with clients and doctors are carried out as needed according to the situation in the city, due to restrictions on movement and changes in the schedule of sites. Clients are interested in whether the SMT will work, where to get ART, how to go abroad, and where to get treatment in another country. Currently, there is a problem with the drug in Odesa oblast (patients have had their dosages reduced), private websites have closed, and the state has been unable to accept new patients.
In Kryvyi Rih, some program activities of partner NGOs have been suspended to assist key groups in coordinating evacuations and meeting their urgent needs, including humanitarian aid. Most documentaries noted that the war made significant adjustments to the rhythm of life. However, some issues began to be addressed more quickly, and clients applying for the Project’s services became more responsible. The format of work and provision of services to the clients of the Project remained almost unchanged. In addition, the documentaries noted that war disciplines and awakens humanity. For example, the number of cases related to stigma and discrimination against PWUD, SP, MSM, and PLHIV by health workers has decreased.
In Ternopil there is anxiety and depression among both the team and customers. Most often, there are appeals from SMT clients (mostly from Kyiv) who received drugs at their own expense, and now doctors in Ternopil do not want to accept them for government programs and send them to other regions, explaining that their clients do not have enough drugs.
“In such a difficult time, we want to pay full and as much attention as possible to everyone who asks for help and to be useful. The priority is just a kind word and a friendly attitude to those who need it”, – Kozaretska Tetyana, coordinator in Ternopil region.
In the Ivano-Frankivsk region, work has increased much since the beginning of the war due to the provision of services to people who have been forced to leave their homes and currently live in the region. All work went into 24/7 mode. There are various requests from community representatives: from requests for food and medicine to consultations on going abroad and receiving ART or SMT both abroad and in the region. If the cases occur in other oblasts or districts, they try to refer the person to social workers nearby and provide telephone consultations. In addition to the main work of support and assistance to clients, the work today is very similar to the work of hotlines or counseling centers. The documentaries note that communication with government agencies in Ivano-Frankivsk Oblast has deteriorated as many structures have now become focal points for IDPs. But doctors are understanding, trying to help more than before.
“The last case was addressed by a drug addict, who, according to him, was in Kyiv on the paid SMT website, and he does not know whether he was registered at all, in our region he was immediately accepted for the program,” said Svitlana Demyanchuk, coordinator in Ivano-Frankivsk. Frankivsk region.
Quite often in Ivano-Frankivsk oblast, there are complaints about violations of citizens’ rights regarding forced mobilization of HIV-infected and drug addicts to the Armed Forces of Ukraine; committing domestic violence against women living with HIV; failure to provide SMT in penitentiary institutions. Complaints are received from IDPs alleging that CNAP staff do not apply for monthly payments to adults and children when registering and obtaining an IDP certificate.
Despite the difficult working conditions today, the regional coordinators note that attention is paid to all people who seek help. It is important to organize work in detail in all directions in order to keep people alive, although sometimes it is very difficult to create safe conditions. It helps to support a large number of friends, colleagues, acquaintances, experts and volunteers in various fields. The work of the Project is currently very relevant and is in great demand among both clients in the region and among IDPs. Due to the high percentage of population migration, documentarians have to perform many additional functions.
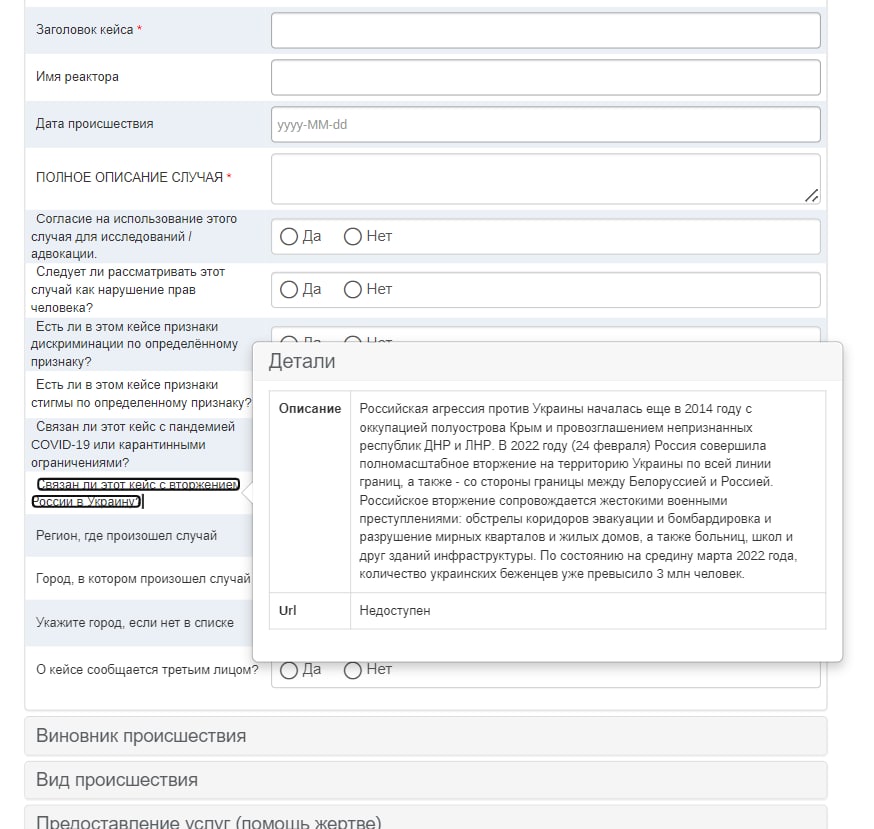
On February 24, 2022, Russia carried out a full-scale invasion of the territory of Ukraine along the entire borderline, both from the Russian Federation and from the Republic of Belarus.
The Russian invasion is accompanied by such brutal war crimes as the shelling of evacuation corridors and humanitarian convoys, the bombing of peaceful neighborhoods, residential buildings, hospitals, and other infrastructure buildings, etc. In this regard, about 3 million Ukrainians were forced to leave their homes and go abroad to seek salvation.
It is in such difficult times that the work of the REAct project becomes even more necessary and in demand. Based on today’s conditions, we managed to quickly reformat the system of work of the REActors and partially change the scope of assistance to Ukrainians for their further protection.
Every Ukrainian who was forced to leave the country, and not just representatives of the HIV and TB communities, can report a violation of their rights and receive free assistance.
We have created a group of specialists who will be able to remotely assist or advise Ukrainians on the protection of human rights abroad as soon as possible. These issues include violence, human trafficking, stigma and discrimination, denial of services, etc.
One can report a violation and get free help by leaving a message in one of the REAct chatbots, updated in accordance with the conditions which each of us suffers today.
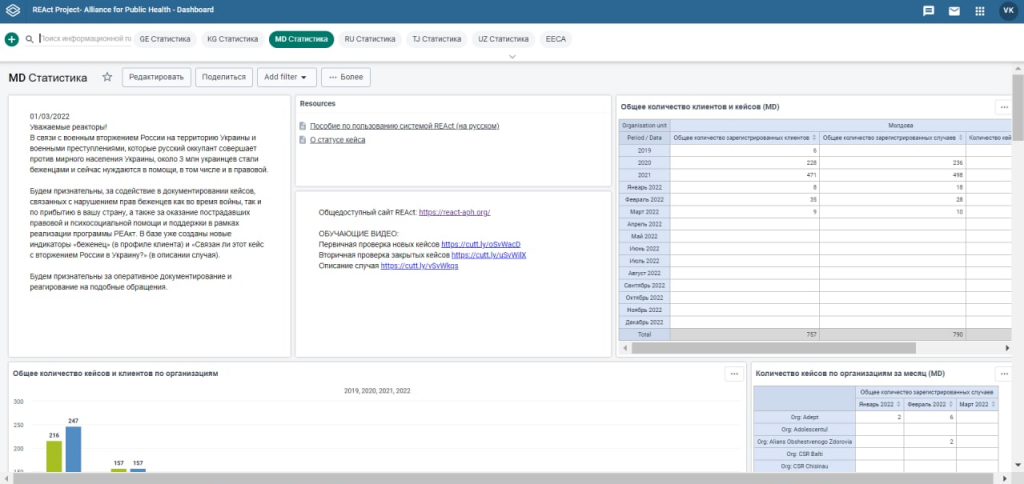
In addition to Ukraine, other countries that implement the REAct tool have also rebuilt their system of work. Among such countries are Moldova, Georgia, Kyrgyzstan, Uzbekistan, and Tajikistan. Moldova has already begun to document cases not only of its own citizens but cases of violation of the rights of Ukrainians on its territory. To this end, we have adapted the REAct database, adding new fields and questions that provide further qualitative documentation and analysis of the specifics of human rights violations among refugees who ended up in countries of influence of the REAct system.
Such international cooperation allows one to get not only remote assistance but also rapid response and provision of services on the ground. In addition, such a system allows the REActors to work together and find the most optimal ways to solve the problems of Ukrainian refugees as soon as possible.
In early November, Oksana got a fever and had trouble breathing. After a week of this condition, she decided to take a test for COVID-19, but the result was negative. The girl lay in this state at home for a week. Despite taking a bunch of drugs, her condition became worse and worse.
An ambulance was called and the client was taken to a local hospital. After a CT scan, the doctor diagnosed her with pleurisy and left her to continue treatment. A few days passed and the doctor found out that Oksana had HIV-positive status.
The man came to the girl’s ward and told her to pack up and go to “her” hospital for treatment, where everyone with HIV status is examined. The client explained that there is no such hospital, so she has nowhere to go.
No arguments and pleas convinced the doctor. With a high temperature, he put Oksana outside the door. The girl called the REAct documentary and she arrived at the hospital. The head of the department was categorical and told the staff of the department to discharge the client from the hospital because she was HIV-positive. Thus revealing her status to all patients of the ward and others.
After that, the documentary of the Project wrote a complaint to the chief physician of this medical institution and called the hotline of the Ministry of Health, leaving an oral complaint about this case. Then Oksana was referred to friendly doctors in another hospital, where the girl arrives to this day.
A PLHIV turned to the REActor for advice and a request to help resolve the current situation in relation to her minor daughter, who also has an HIV-positive status.
The woman and her daughter came to their family doctor in order to draw up medical documents for the child to visit a holiday camp. The doctor completed the necessary documents and gave them to the woman, on the title page of which the client saw the inscription “B-20”, which means that the owner of this document is PLHIV.
The woman asked the medical worker to take away the inscription since it is a disclosure of HIV – the status of a child and is considered an offense. However, the doctor refused to do so.
The client turned to the employees of a friendly NGO to help her resolve the situation. The social worker of the organization, together with the client, went to the family doctor, where the documenter held an explanatory conversation with the medical worker, spoke about the criminal liability for her actions and about the regulations that the doctor violates. After that, the inscription on the child’s document disappeared and the social worker secured the doctor’s promise that such situations would not happen again.
To further explore the subject of medical care for prisoners, let us review the specific forms of medical care that should be made available to incarcerated individuals as well as the particular requirements that the administrations of correctional facilities of the State Penitentiary Service of Ukraine (SPS) are obligated to comply with to make sure that relevant arrangements are in place.
Mandatory preventive health assessment of prisoners.
With a view to detecting and preventing the spread of infectious diseases, as well as identifying general medical conditions and mental disorders among incarcerated individuals held in SPS correctional facilities, inmates must undergo an annual preventive health assessment, whereas juvenile (minor) detainees and prisoners held in cell-type settings have to undergo such an assessment on a biannual basis.
The following physicians have to be involved and take part in a preventive health assessment:
– general internist (or general practitioner/family doctor);
– psychiatrist;
– dentist.
If there are no such specialists available in the medical unit of the correctional facility concerned, they have to be procured by the correctional facility’s administration from SPS-controlled or other health care facilities.
Outpatient medical care for prisoners.
Outpatient medical care for incarcerated individuals should be provided by the designated medical worker of the correctional facility daily during the hours scheduled by the head of the medical unit (paramedic station) and approved by the facility’s administration. Escorted by a correctional officer, inmates who have been prescribed outpatient treatment have to report to the medical unit for their medications and other procedures during scheduled times during the day. Normally, prisoners have to take their medicines in the medical unit as prescribed by the doctor and under the supervision of a paramedic (physician assistant). However, if, based on medical needs, these medications are supposed to be taken around the clock, the dispensed medications must be handed over to the prisoner.
Inpatient medical care for prisoners.
Incarcerated individuals might need hospital care from the medical unit for the following purposes:
– health assessment and treatment of prisoners in need of inpatient care for up to 30 days;
– medically necessary inpatient treatment of prisoners discharged from SPS-controlled or other health care facilities;
– temporary isolation in the infirmary (isolation ward) of the medical unit for infected or suspected patients before referral to a specialist hospital;
– inpatient treatment of non-transportable cases until their condition becomes stable before referral to a SPS-controlled or other health care facility.
During the stay in the hospital section of the medical unit, incarcerated individuals must be examined and evaluated based on their existing medical condition across all instrumental and laboratory research options available in the medical unit concerned.
Referrals to healthcare facilities for hospitalization shall beprovidedto any prisoners who have become ill or experienced an acute exacerbation of the chronic disease, which requires inpatient treatment in SPS-controlled health care facilities (or, if services are unavailable and under a certain set of circumstances, said patients can be referred to general-public health care facilities), including situations when some additional examinations needed cannot be performed by SPS health care facilities (if they are outside of the scope pre-determined and require equipment, laboratories, or medical care other than that available on site).
Emergency medical care for individuals detained or sentenced to imprisonment is provided by the medical staff of the relevant SPS-controlled health care facility, or, if it is impossible to ensure the full scope of services needed, by the emergency (ambulance) team of the center for emergency medical services located in the administrative division (geographic area) where the correctional facility or pre-trial detention center is situated.
The administration of the correctional facility or pre-trial detention center where the inmate concerned is held shall be obligated to immediately summon an emergency ambulance if required and requested by the medical worker of the SPS-controlled health care facility.
If the emergency ambulance crew should decide that a prisoner needs to be hospitalized, they will be transported to the relevant health care facility by the ambulance crew concerned. In this case, the administration of the correctional facility or pre-trial detention center in question must put in place and ensure appropriate guarding and security arrangements.
Recently a REActor reported a problem that is currently quite common for Ukraine. Viktor, who is an OST patient, was stopped by the police without due cause while driving.
After being forcibly pulled over, he was sent to the designated testing lab for drug tests. Once the presence of OST drugs (methadone) in his system was confirmed, the doctors concluded that the man was driving under the influence of the substances identified. Based on applicable regulations and policies, this in turn is punishable by administrative penalties and suspension of driving privileges.
Viktor filed an appeal to the administrative court, which identified procedural violations in breach of drug testing regulations and standards and overturned the decision regarding administrative liability penalties. It later transpired that Viktor’s personal data had been improperly entered into the ARMOR police database records, thus making him a target for police prosecution efforts.
The REActor is currently taking all necessary steps to have Viktor’s personal data removed from the database. Appropriate petitions have been made to responsible officials as well as to the Ombudsman. Resolving this problem will make it possible to reduce the level of bias and stigma against members of vulnerable communities.
Unfortunately, in today’s Ukraine, the number of types of addictive behaviors tends to consistently increase and, accordingly, so does the number of people with various forms of addiction. We live life “the way we want to live it,” asserting ourselves at any cost and by any means whatsoever.
Researchers distinguish four forms of dependent behavior, perceived as a departure from reality:
Escape into the body – the aspiration to achieving unlimited physical or mental “self-improvement” goals;
Escape into work – excessive focus on job- or education-related agendas;
Escape into interpersonal contacts or solitude – a constant desire to communicate with others or, conversely, seek solitude;
Escape into fantasy – living in a world of illusions and fantasies.
Each of these behaviors can be achieved or accompanied by the use of alcohol, drugs, toxic substances, and non-chemical addictions (e.g., Internet addiction, gaming/gambling addiction, etc.).
The addicted person feels an irresistible craving to experience intense emotions by artificially altering their mental state through the intake of certain substances or being constantly fixated on certain activities. The desire to escape from reality is a normal state of mind for people like this.
Chemical addictions (dependence, bad habit, addiction) are characterized by a person’s consistent ingestion of psychoactive substances, and an irresistible urge to regularly use the substance of choice while experiencing significant difficulty breaking the habit without outside help.
The object of dependence in non-chemical addictions is a behavioral pattern (model, mechanism, behavior). Non-chemical addictions may come in the following forms: pyromania, kleptomania, gambling (gambling addiction), computer or Internet addictions, relationship addictions, sexual or love addictions, workaholism, addiction to spending money, listening to rhythmically accentuated music, exercise addiction, addiction to spiritual practices (spirituality), lust for power, addiction to joyriding (Toad’s Syndrome), etc.
One of the major reasons for addiction is addictive-type personalities seeking to change their lifestyle, which is often described by them as “drab,” “boring,” “monotonous,” “apathetic,” “heartless.” There are several key types of motivation for using alcohol and drugs, i.e., the factors that drive chemical addictions.
1. Motivation driven by the desire to alleviate or eliminate emotional discomfort (emotional distress, fear, anxiety, etc.).
2. Hedonistic motivation – if the example above is driven by the desire to restore emotional balance after being at a low point (loss or disappointment), then hedonistic motivation is intended to improve the mood that is normal (not at a low point). The hedonistic focus is manifested in an urge to chase after pleasure, experience feelings of joy.
3. Motivation to activate a behavior – psychoactive substances are primarily taken not so much as to produce euphoria, but to trigger activity. Addicted individuals try to bring themselves out of a state of passivity, indifference, apathy, or inactivity with the help of substances that provoke larger-than-life, extremely vivid reactions and pursuits, including risky behaviors. For example, the intake of psychostimulant drugs can stimulate sexual activity and produce a “record performance” in terms of sexual prowess.
4. Motivation aroused by pressure from others – this reflects the inability of a person to say no to alcohol or drugs being offered by other people and is accounted for by dependent-personality traits (timidity, shyness, submissiveness, anxiety, being overly wary and circumspect in interpersonal communication settings), with the result that the individual seeks to avoid social situations exposing them to harsh judgment (specifically, for declining an alcoholic drink, rather than “going along to get along” and drinking it just to be social).
5. Pseudocultural motivation – based on the person’s world outlook and aesthetic sensibilities. The person considers the consumption of alcohol or drugs through the prism of “sophisticated taste,” as a hallmark of belonging to the in-crowd. It is not the use of substances that matters here, but the demonstration of this process to those surrounding you.
Most addicts suffer from being different in that they are “unable to live like other people do.” This may be manifested in the fact that some addicted individuals have to adjust to societal norms, play the role of a “friend among foes,” perform the social roles imposed on them by society (e.g., a model son, a virtuous fellow worker, etc.).
There is a multitude of scientific concepts that attempt to explain how chemical dependencies emerge (genetic, genetotrophic, ethanolic, adrenochromic, endocrinopathic, bioenergetic, etc.). That being said, we will focus on the main biological and social factors that drive the development of dependence on psychoactive substances.
Biological factors include the following:
1) Heredity (biological inheritance) – the child of parents who use drugs is born with a low tolerance to the drug in question and high sensitivity, therefore, even the first small dose of it will cause the maximum effect, thus accelerating the formation of dependence on the psychoactive substance concerned;
2) Sex – the female body is more sensitive to psychoactive substances than the male body;
3) Weight – there is an inverse relationship between weight and susceptibility to drug addiction;
4) Age – the enzyme system that absorbs and processes the drug is at its most vulnerable in adolescents and the elderly;
5) Health status – the “aggravating” factors here include: pathology of pregnancy and complicated childbirth; severe and chronic childhood diseases; cerebral concussion;
6) Tolerance – individual resistance (sensitivity) to relevant chemicals. Over time, tolerance first increases due to the faster metabolism of the drug, then it decreases.
Social factors may include:
1) Family – the tendency to use psychoactive substances is contributed to by: parental alcohol abuse or drug addiction; parental psychotic disorders; tragic events within the family (for example, the suicide of one of the parents); forced separation from a person if there was a strong emotional attachment involved; loss of the role of “family hero,” the position of “Cinderella” due to a change in family structure (the appearance of a stepfather/stepmother, half-brothers); a “family disaster,” which dramatically altered the adolescent’s social and psychological status; constant parental conflicts; upbringing in a single-parent household; one parent being unavailable due to a busy schedule (long business trips, work overload); there being no other children in the family; “rebellion” against excessive control by parents and other family members; domestic abuse.
2) Informal group – being around friends who use alcohol or drugs. This mechanism is especially important if the atmosphere at home is not good if there are conflicting relationships between parents and children, physical violence in the home, low emotional attachment to parents, poor family cohesion.
3) Educational and professional groups – individuals tend to initiate substance use / often use psychoactive substances in educational or professional settings.
4) Availability of drug substances;
5) The impact of the macro-environment – an unstable economic situation, a drop in living standards among the majority of the population, significant unemployment levels, “social depression,” a perceived lack of personal prospects, and having a low sense of self-worth.
6) Flippant attitudes spread by ill-conceived media information campaigns arouse an unhealthy interest in the consumption of psychoactive substances and a sense of social endorsement.
Rights violation incidents recorded by the REAct project often include failure to provide medical care to incarcerated inmates in detention and prison settings. Correctional officers do not respond appropriately to prisoners’ requests, arguing that “jail/prison is not a spa resort.”
However, applicable regulations require that individuals sentenced to imprisonment have the right to health care within the scope prescribed by the Law of Ukraine on Health Care, except for certain restrictions expressly provided for by law. Responsibility for the health of prisoners rests with the administration of the correctional facility concerned, as well as employees of facilities that report to the Health Center of the State Penitentiary Service of Ukraine (SPS).
Convicted individuals have the right to seek professional advice and treatment both in the medical facilities of the Health Center of the State Penitentiary Service of Ukraine, which operate in relevant correctional settings and must provide free medical services to incarcerated inmates and in any other health care facilities licensed by the Ministry of Health of Ukraine, including private ones. The costs of related services and medicines to be purchased in this case should be covered by prisoners, their family members or friends at their own expense.
The Right to a Free Choice of Physician.
Any prisoner has the right and is free to choose from among qualified physicians, health care facilities, or treatments based on the recommendations provided. Convicted inmates or their relatives have to contact the chosen medical practitioner and, once their consent is obtained, inform the correctional facility’s administration of the scheduled date and time of the appointment.
The algorithm to be used here is as follows: the convicted prisoner contacts the physician of the SPS health care facility and asks for an appointment with the chosen doctor. Within 24 hours thereafter, this physician must prepare a medical opinion and file a request to the facility administration for permission to allow the chosen doctor to see the patient. This request must be approved by the head of the SPS health care facility in question.
In this case, all expenses related to the provision of paid medical services (including those provided by the chosen doctor), as well as the purchase of medicines, medical devices (patient care items), technical and other equipment for rehabilitation, are outside the scope of public funding, shall be borne by the convicted inmate (recipient of care), their close relatives, or other parties involved. The medical opinion will serve as the grounds for providing the medical care requested.
The Right to Be Examined and Treated in Other Health Care Facilities.
If any additional examinations needed cannot be performed by SPS health care facilities (e.g., if they are outside of the scope pre-determined and require equipment, laboratories, or medical care other than that available on site), such examinations should be carried out by another health care facility where they may be performed, within the time frame specified in the medical (opinion) report.
If inpatient treatment is required, the convicted inmate has the right to contact the physician of the SPS health care facility requesting that medical assistance be provided by another health care facility that has the capability to provide the necessary medical services both at public expense and at prisoners’ own expense. The physician of the SPS health care facility must consider the request and draw up a medical report with their professional opinion on the matter at hand no later than the next working day after the request is made.
Access to Medicines.
Convicted inmates have the right to be provided with free medicines in SPS health care facilities, which are available or should be made available. If a prisoner wishes to use some other medical supplies for their treatment that are not available in a health care facility (medical unit) within the correctional system, the same can be obtained from family members based on a medical opinion from the physician of the correctional facility. Prescribed based on the medical opinion, the medical drugs thus obtained are not handed over to the prisoner per departmental regulations and policies, but transferred to the SPS health care facility for the prisoner’s treatment. The incarcerated inmate will be offered to take these medicines only in the presence of the designated medical worker of the SPS health care facility. The only exceptions are medications necessary to maintain the prisoner’s vital functions. All medicines must be in standard undamaged factory packaging.
The convicted inmate’s family members or other persons involved are required to submit an application for the transfer of said medicines, medical devices (patient care items), technical and other equipment for rehabilitation. The application form must be attached to the prisoner’s medical record. Once the care package containing the items required is delivered, the prisoner has the right to review the itemized list of contents enclosed (medicines, medical devices (patient care items), technical and other equipment for rehabilitation intended for his or her treatment), confirming this by their signature on the application form. Medicines and medical devices (patient care items) provided by prisoners’ family members or other persons involved shall be stored by SPS health care facilities in separate cabinets and listed in the record log for medicines, medical devices (patient care items), technical and other equipment for rehabilitation received from prisoners’ family members and other persons involved. Prisoners are required to sign the log after the completion of the treatment course and have the right to monitor the use of their medical drugs.
Inna turned to the REAct project for help complaining about her rights being violated. The girl was refused registration as pregnant for prenatal care at the maternity welfare center due to her HIV-positive status. Moreover, Inna was referred to the local AIDS center instead, where the service required was not even available.
Following the REACtor’s intervention, it was explained to the gynecologists at the center that their actions were discriminatory because it was against regulations to divide pregnant women into categories based on their health status, thus making a distinction between “HIV patients” and “those who are well and healthy”.
Additionally, the maternity welfare center’s authorities were reminded that Inna had the right to sue them over the refusal to register her. Only after hearing these arguments did they offer their apologies to the girl and provide the service needed.
Halyna is a woman who is HIV-positive. After giving birth, she approached the district pediatrician asking to be provided with free milk formula to bottle-feed her newborn baby. Even though this situation was covered by a set of mandatory measures intended to prevent vertical transmission of HIV from mother to child, the woman’s request was denied on the grounds that the local budget had no allocated funds for providing prevention supplies.
Halyna turned to the REActor for help. The woman was assisted in accessing psychological support and legal advice. Additionally, the REActor helped her draft a written request to the regional health department. Concerted efforts ensured that the woman was provided with food vouchers and milk formula for her baby, related expenses being covered by a partner organization.
Iryna filed assault and battery charges at the local police station. The officer who took the statement was dismissive of the girl and the situation at hand because Iryna looked unkempt and untidy, and had TB.
Although the statement contained specific details about the person who had committed the beating, as well as about the witness to the incident, Iryna was assured that the situation did not include all essential elements of the offense charged, and advised to take the matter to court as a civil law case.
The girl went on to seek help from the REActor, who provided Iryna with a list of documents that are required to apply for free secondary legal assistance, as well as offered guidance and advice on the steps to follow, should a situation like this arise again in the future.
Later on, a counselor at law was assigned to the girl’s case at public expense, and proceedings were initiated to address the failure to enter information about a criminal offense into the Unified Register of Pre-Trial Investigations.
Denial, resistance, and sabotage are frequently encountered in response to an attempted offer of help in these situations. The deeper the denial, the stronger the resistance. It can manifest itself in refusing to undergo treatment for addiction, or in the apparent sabotage that undermines the care being provided.
Psychotherapy for codependency is targeted at achieving behavior change and readiness to make the changes needed. It is human nature to seek stability. This is a safety issue. Any stability, for good or for bad, is better than something unknown. But any change intrinsically carries a risk. Therefore, change is considered a threat.
When we are in danger, we experience fear. Fear is a very unpleasant emotion that we try to avoid. If this experience cannot be avoided, then we seek to get rid of it. Our internal defense mechanisms can shield us from fear. The three primary defense mechanisms used unconsciously are the fight (anger), flight, or freeze responses. They all manifest themselves in different ways.
Thus, in psychotherapy for codependency, any change in a codependent person’s life is viewed by them as a risk, and perceived risk causes fear. Therefore, psychotherapy (“treatment”), in the opinion of a person who is codependent, is something to be afraid of.
Anger is manifested in overt resistance and sabotage in response to the offer of help as well as statements to the effect, “How can this help me?!” or “This won’t help me!” The client may shout and openly express their nervousness through words or non-verbally; they may give their personal reasons and examples that justify their current life situation. According to the client, the proposed course of action will in no way benefit them. For example, the idea of spending one hour a week attending a codependency self-help group may cause a storm of protest from a mother whose son has drug addiction issues. This is despite the fact that prior to psychotherapy this woman may have spent years and countless resources searching for a “cure” for her son.
Of course, not everyone who is codependent reacts so vehemently to the offer of effective help. But few agree to receive effective help the first time it is offered. Even after giving consent and attending a self-help group once, most codependents conclude that this strategy does not work. And they feel outraged and anger, thinking: “This psychotherapist might have offered something better for me instead!”. There are no valid arguments, even when supported by examples or evidence, that will convince a person who is in denial.
Many codependents demand that psychotherapist should turn their lives around overnight. It seems to clients that one or two sessions of therapy may result in radical life-changing outcomes and, most importantly, that their chemically dependent family member will get fully recovered after that. And if they do not see this happening, they conclude that psychotherapy does not work!
Self-deception or partial consent on the part ofthe codependent person isa noteworthyphenomenonto explore: “Okay, I will partially do as you’re suggesting, but on my own, without discussing anything with the therapist, after introducing some / major adjustments to the recommendations.” And this kind of reaction is understandable because change is scary. This is especially frightening when the addicted person demonstrates overt aggression toward the codependent. For example, some addicts openly resist, throw fits and make scenes, or even forbid their near and dear ones from attending self-help group meetings, calling them a “sect” or labeling their family members as “crazy.” Therefore, changes involved in the process of psychotherapy are objectively risky and may draw forth unpleasant reactions and responses from the addicted person. It is important to have the courage to take the plunge and follow through with them.
It is difficult and sometimes impossible to recover alone. Therefore, help for codependents should be underpinned by group support, the main tool here being mutual support.
The freeze response is just a reaction when a passive stance is assumed: “If I don’t do anything, nothing bad is going to happen.” But we know that this is not the case, because chemical dependence (and hence codependency) always progresses gradually over a period of time. So, unless some steps are taken about it, the situation will only get worse.
Thus, psychotherapy for codependents is directly related to risk. It is quite difficult to make the decision and go through with it, but it is a necessary step. In order to take risks, you need to be willing and prepared to deal with them. And keep this pattern in mind: the fewer problems there are, the less the codependent wants to change anything. But the more problems there are, the harder it will be to change something!
Petro has HIV+ status and has been in the penitentiary facility for more than two years. During this time, he has never had a CD4 count which may result in interruption of treatment monitoring.
The man contacted a REActor, a representative of a friendly organization “Ukraine without tortures” asking for help in solving this issue.
To maintain confidentiality, the REActor approached the head of the healthcare site with a request to perform such testing to all theimprisoned PLWH upon their consent. According to the national and international standards, the state must ensure through monitoring of prisoners’ health and treatment they receive.
In conversation, the head of the healthcare site explained that such tests were not performed due to lack of funding, promising to doanything in his power to arrange testing.
In a month, Petro confirmed that he took the test and was informed about its results.
Lisa contacted a REActor asking to help her with a refusal in medical service provision. A gynecologist in the oblast hospital refused to perform laparoscopic surgery for ectopic pregnancy and insulted the girl by making insinuations about her HIV status.
The REActor consulted Lisa and explained to her all the mechanisms of protecting her rights. In addition, the girl was proposed assistance in obtaining medical care. Together with the client, the REActor visited the Head of the Oblast AIDS Center to discuss this issue. The doctor promised to take this case under her personal control. The surgery was performed free of charge due to the call to the Ministry of Health hotline.
According to various data, the number of people who inject drugs exceeds 300 000 persons. Addiction to drugs is a problem turning into a tragedy both for the affected individuals and their families.
Individual civil society initiatives do not solve all the problems. The statistics of people who inject drugs demonstrate the need for an effective comprehensive approach.
An online discussion “A drug trap: How to help the families of drug users” was held on December 22. The participating experts were Maksym Butkevych, expert of the REAct system in Ukraine; Tetiana Koshova, President, Charitable Fund “Hope and Trust”, the NationalHotline on drug addiction and OST operator; Volodymyr Kurach, Head, Center of addiction treatment “TACTICS”, civil society activist.
The activity was held in relation to the screening of the movie “The Little Samdi” in the DOCUSPACE online cinema on the agenda of the 18th Docudays UA International Human Rights Documentary Film Festival.
After contracting COVID-19, Anna regularly complained of feeling poorly. She decided to see her family doctor to be examined and, if need be, receive treatment. However, as soon as the patient informed the medical practitioner about her HIV-positive status, the woman physician refused to provide medical help to Anna, her reasons being that she was “contagious” and not supposed to be among “normal people”. The doctor advised the client to seek help from the AIDS Center because she was not paid any extra compensation for dealing with “contagious” patients.
Understandably, the patient was outraged and insulted by this doctor’s attitude and behavior, which prompted her to seek help from the REActor based in a partner NGO. On the day she reached out for help, the client was assisted in accessing psychological support and escorted by a social worker to another health care facility, where the patient-friendly doctor duly provided the girl with professional medical guidance.
In addition, a statement was prepared and submitted to the management of the health care facility where the incident occurred to make sure that necessary steps are taken and no other patients have to experience similar stigma and discrimination by health professionals in the future. Following this move, disciplinary action in the form of a reprimand was taken against the doctor concerned. Additionally, other employees had to undertake appropriate training on how to prevent stigma and discrimination as a major barrier to treatment.
Among the violations registered by the REAct project, reports on disclosure of the clients’ health status are outstanding. Such cases may have various consequences, ranging from the feeling of stigma and humiliation to forced relocation caused by denigration and bullying by the local community after HIV status disclosure.
Often, when patients with HIV-positive status are seeking medical care, they are concerned that the health and personal information they report to the physician will become available to third persons, especially in the context of HIV/AIDS? What are the guarantees of protection and how to use them?
The Law of Ukraine “The fundamentals of the legislature of Ukraine concerning healthcare” (Art. 39-1 and Art. 40) envisage the right to the confidentiality of the health status, the fact of seeking care, the diagnosis, and the findings of medical examination. Employers and schools are prohibited to request information on the diagnosis and treatment methods, as well as provision of such information upon such requests. It is highlighted that health professionals and other persons who, in performance of professional or official duties, became aware of the disease, medical examination, and its findings, the intimate and family life of the individual, do not have the right to disclose such information, except cases defined in the legislature. The Law of Ukraine “On preventing the dissemination of diseases caused by human immune deficiency virus (HIV) and legal and social protection of people living with HIV”, and other regulations envisage some guarantees of the right to medical confidentiality in the context of HIV.
What you need to know about medical confidentiality
All information related to somebody’s health and health-related circumstances is subject to medical confidentiality.
Including:
The fact of seeking medical care in a health facility;
Health assessment results;
Medical diagnosis;
Circumstances preceding or provoking the disease;
Individual characteristics of the organism;
Bad habits, mental characteristics and income status;
Other information received during the medical visit, including information about family and intimate life, the health status of relatives and close people.
Physicians, nurses, other clinical and non-clinical staff, who, in performing their duties, became aware of the disease, do not have the right to disclose clinical and non-clinical information related to the person’s health status. Such information can be disclosed to a person authorized to receive such information, exclusively in cases envisaged by law, with compliance to all regulatory requirements ensured.
When can a doctor disclose medical confidentiality and under what circumstances?
Disclosure of information about a person’s positive HIV status to the person’s partner by health professionals is allowed in cases if the person living with HIV, gives relevant written authorization, or if such person has died, fainted or there is a likelihood that such person will not regain consciousness and recover his/her capacity to provide informed consent.
Sharing such information with other health professionals and health facilities is allowable only upon informed consent of the person living with HIV, for sharing such information. Such consent must be provided in writing and only for the purposes of treating the diseases caused by HIV and in a case if a physician’s awareness about the patient’s HIV status makes a significant difference for treatment.
Sharing such information with other third parties is allowed only upon a court decision in the cases defined by law.
“Other third parties” imply the inquest and investigation authorities and the court, and “cases” mean the criminal proceedings regarding the person or other legal grounds. It is important to know that sharing any confidential health information with the inquest and investigation authorities implies exclusively legal and procedural access to it. Access to such information is granted on the basis of Art. 162 of the Criminal Procedure Law of Ukraine and Art. 160, 163 of the Criminal Procedure Law of Ukraine governing the order of obtaining temporary access to things and documents containing legally protected secrecy based on the relevant request reviewed by the investigating judge.
This means that any efforts of, for example, police officers to access such information in other ways are unlawful and must be ignored by the healthcare staff.
The liability for disclosing confidential health information by healthcare workers is envisaged by Article 145 of the Criminal Code of Ukraine “On illegal disclosure of medical secrecy”. According to Article 132 of the Criminal Code of Ukraine, disclosure by a health facility official, a support employee who had unauthorized access to information, or another healthcare worker of information about medical examination of a person to detect human immune deficiency virus infection, or other incurable life-threatening infectious disease, or acquired immune deficiency syndrome and its outcomes which became known in the course of performing official or professional duties, is also subject to criminal liability.
A person who was harmed by restriction of his/her rights as a result of publicization or disclosure of his/her HIV status is entitled to file civil proceedings against the perpetrator claiming reparation according to Article 15 of the Law of Ukraine “On preventing the dissemination of diseases caused by human immune deficiency virus (HIV) and legal and social protection of people living with HIV”.