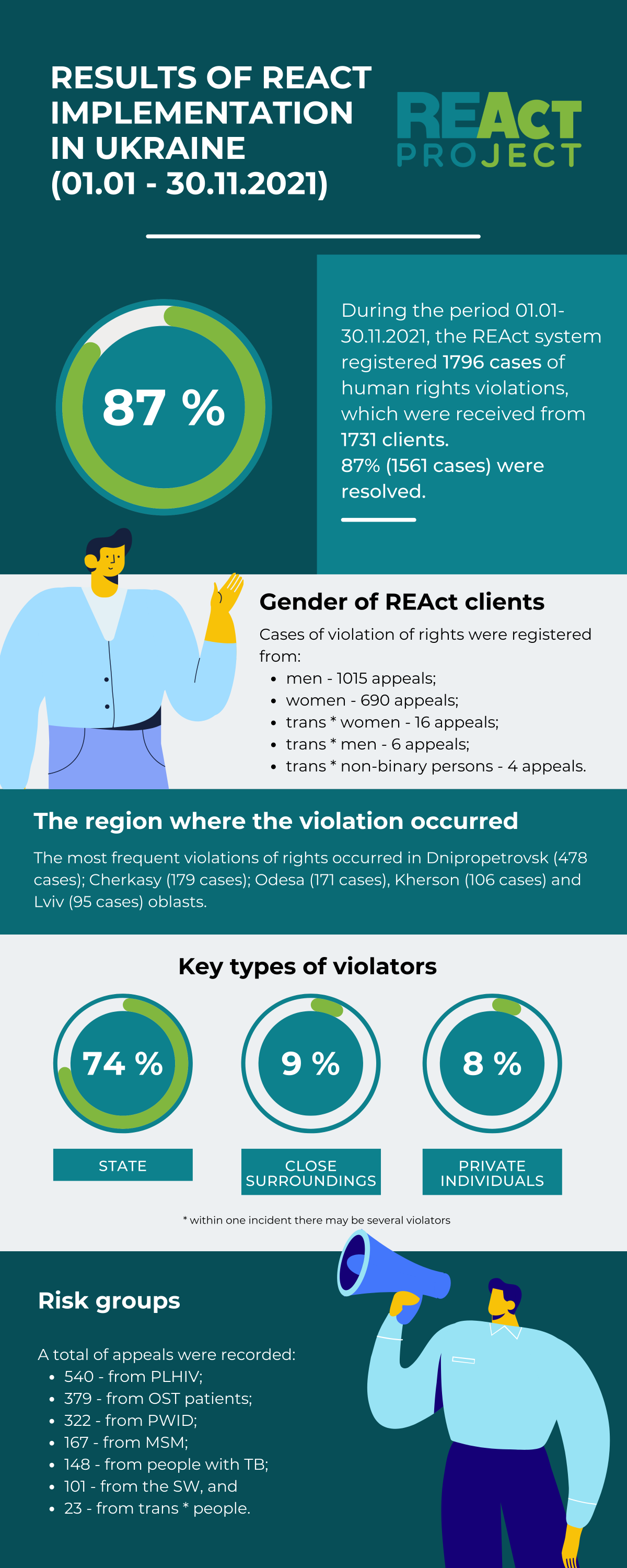
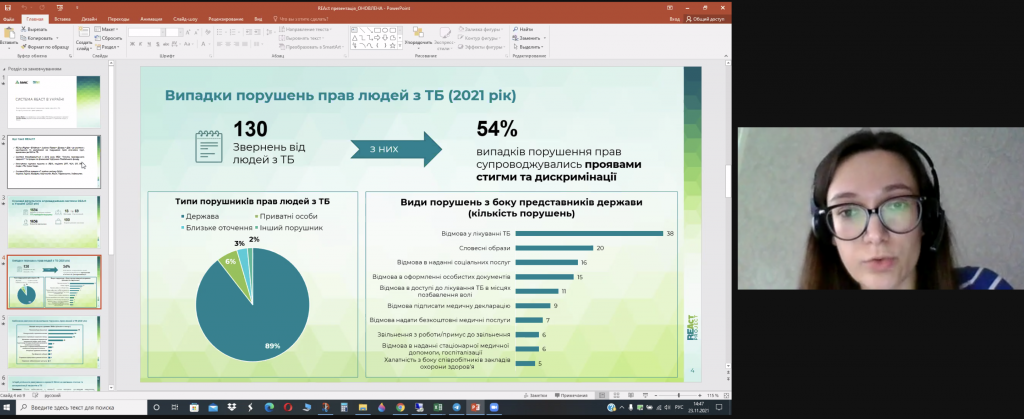
In 2021, the REActors registered multiple cases of violation of the rights of OST program clients. Such violations included interruptions in essential drug supply and illegal detentions of OST program clients by law enforcement authorities. In January – November 2021, 379 OST program clients reported violations to the REAct system.
On the International Solidarity Day commemorated on December 20, Ivan Viktorov, REAct coordinator in Kyiv oblast, tells about the difference in receiving OST in public and private OST sites, possible causes of interruptions in drug supply, their consequences for the clients of private OST sites, and about the role of non-governmental organizations in protecting the right of key populations to receiving vital treatment.
- Receiving OST in public OST sites under OST program and in private facilities, for example, through pharmacies – what is the difference, advantages and risks for the clients?
The difference is that the client receiving OST medication with a prescription in a pharmacy does not need to adhere to the schedule of issuing OST drugs, while the state program has certain requirements for the patient. According to the routine OST administration order, the client must visit the OST site at a scheduled time on scheduled days to pick up medications. Another possible mechanism is issuing OST drugs for self-administration for a 7–10-day period. But there are certain eligibility criteria, too: the client must be registered with a state OST program with a conventional OST drug administration schedule for no less than 3 months (in context of the quarantine; earlier this term was 6 months – editor’s comment). This requires the client’s physical presence at the OST site, limiting their free time. For example, for employed clients, this requires them to be absent from work, and the employer may find this an issue. Therefore, people buy prescriptions and pay for medications to live without certain obligations.
- How many clients are enrolled with state OST program and how many receive medications in private OST sites? What is the statistics in Kyiv?
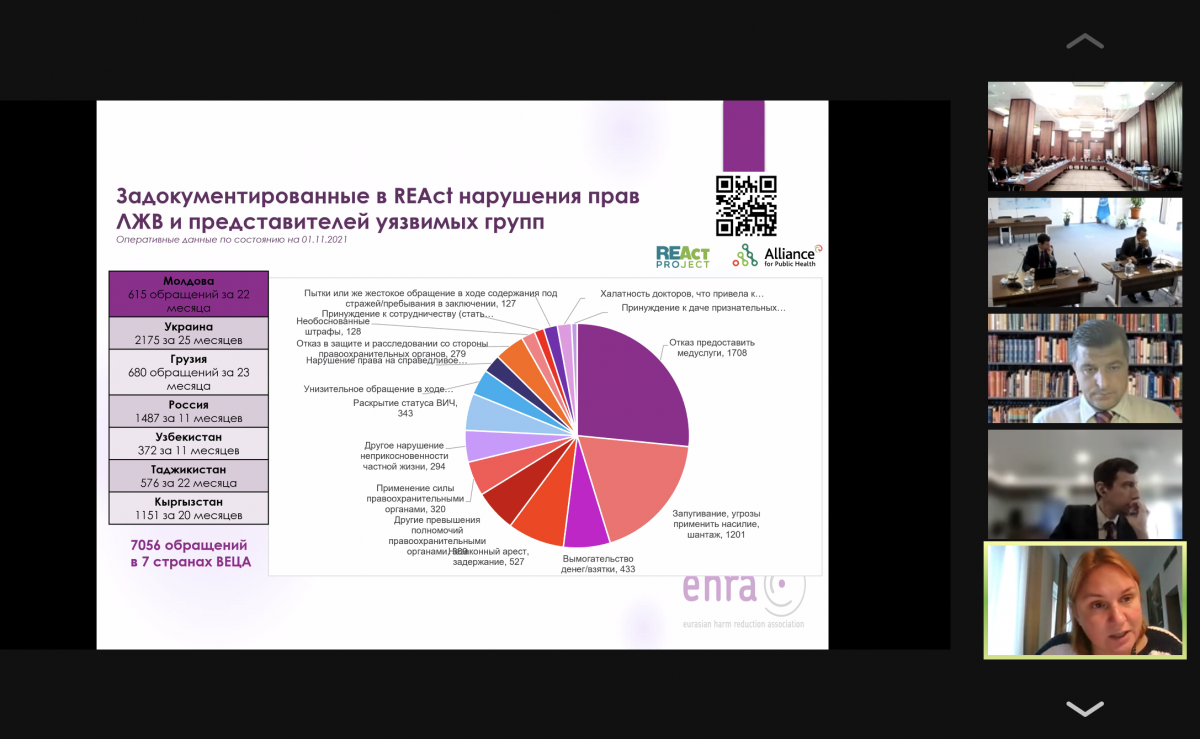
The statistics on public OST sites is available from Ukraine’s Center of Public Health website (as of 01.11.2021, 16 617 persons receive OST services in health facilities – editor’s comment); as for the private sites, I can only estimate: there are about 70 OST sites in Kyiv, each serving about 400 clients. So, the total number of private OST clients is about 20 000. One patient can be registered with several private OST sites. This increases the risk that these drugs are then privately sold. The private OST sites have no shared database to trace the clients already registered with the program. A patient comes to the site, pays, and gets the prescription.
- Which barriers do the clients face in receiving OST drugs from private sites?
Methadone is not always available in pharmacies, so the private OST sites cannot guarantee uninterrupted OST drug supply to the client. Pharmacies can also stir artificial price increase, meaning that later they will be able to sell more at higher prices. There were cases of closure of the OST sites and seizure of all documentation, including the patient’s personal data. Sometimes police officers sweep private OST sites, which does not usually harm the site, but for the patients, it is a risk of disclosure of diagnosis, personal data because often law enforcement officers seize medical documentation (logs, patient files).
- You mentioned instability of receiving OST drugs in private sites. What are the possible reasons for such situations?
First of all, this could be done to transfer more patients to the governmental OST program. But there are several issues: for enrollment with the governmental OST program, the client must be registered in the internal OST client registration system, and this can prevent getting “a normal job”. Besides, the state program sets a number of requirements for the OST clients that I have already mentioned, and they may not be suitable for everyone. Some may be depressed because this may look like the so-called “drug addict” stigma. Interruptions in drug supply occur, as a rule, at the end of the year. There can be several reasons for it: the substances for OST drug manufacturing are procured at the end of the year due to the allocations; the untimely receipt of funds from regional communal enterprises “Pharmacia”; manufacturing of large quantities of drugs for the state order, including for exporting.
- Is there a mechanism to prevent such situations with treatment interruption due to delays in drug supplies to private OST sites?
No. The private sites cannot guarantee uninterrupted OST supply because no one traces such clients – they issue a prescription, take the money for the prescription, and that’s all. Only public OST sites guarantee their clients’ uninterrupted OST drugs administration, therefore there is no risk of treatment interruption and clients returning to illegal street drugs.
- What are the consequences faced by the OST clients if their drugs are unavailable in the private sites or their supply is delayed?
If the drugs are unavailable in the pharmacy, people will go to the so-called “corner boys” (drug dealers – editor’s comment), but their price will be several times higher. If the addicted person has no money, he/she may commit a crime for the need of medications or go out to the street to get drugs, and this means overdose in 90% of cases. Unfortunately, a person can die in absence of timely care.
- If an OST client wants to shift to the state OST program, how soon can the client be enrolled?
The government today is actively enrolling in the OST program; therefore, the client always has a choice of guaranteed provision of OST drugs. It takes a day to become an OST program client – you just need to bring your chest X-ray results. However, this may take longer, because much depends on the client’s will, how soon he/she agrees to enroll with the state program and the client’s commitment. Secondly, there is a certain procedure set forth in the regulations, according to which the patient must undergo the induction procedure (dose adjustment – editor’s comment). After that, the narcologist explains to the patient the need for the administration of such drugs and the motivation for uninterrupted intake, and then the client is administered OST.
- What is the role of non-governmental organizations in supporting OST patients?
To begin with, there are no social workers in the private OST sites, and their presence is not envisaged. The role of NGOs is in counseling clients on transfer to the governmental program, referral and follow-up of such clients, working on treatment adherence. I believe this is a meaningful contribution. There is an OST Hotline operating in Ukraine where clients from all regions can call to report issues related to substitution maintenance therapy. In the beginning, such issues are quickly addressed by NGOs, then we approach public institutions in power to respond. NGOs take efforts in community mobilization and empowerment, initiate amendments to laws and regulations, but unsolved problems remain. For example, we keep writing about issues in the community, but we are unsure if our voice is heard in some public institutions.
- What are the mechanisms of state control of receiving double quantities of OST drugs (from private OST sites and the governmental program)?
It is rather the responsibility of OST clients who get medications from private OST sites while being registered on the state program. However, if police find out this fact, such actions may qualify as the unlawful acquisition of drugs and their storage. This may have negative consequences for the client (there have been cases). In general, there are no mechanisms to trade duplications of OST receipt.
- In general, what are the cases of police violating the rights of OST clients? How are these cases resolved and in whose favor?
About half of all cases of abuses by police officers registered by REAct system in Kyiv oblast, involve OST clients. Police officers often abuse their official powers regarding OST patients, because they still consider them “drug addicts”. Most common violations include illegal detention, police searches, narcological examinations (sometimes forced), seizure of OST drugs, solicitation of money for alleged non-initiation of criminal proceedings. This is despite the fact that the patients did not breach the law, they had absolutely legal prescription for OST drugs. Partner NGOs immediately respond to such cases which more often are resolved in favor of the patient. Our friendly organizations have highly qualified professionals on staff who have been working with key populations for years and know how to act in different situations. To raise awareness of police authorities in working with key populations, training modules are conducted with the support of the International Charitable Fund “Public Health Alliance” and other partner organizations. The training participants are presented data about violations of rights of key populations collected through REAct.
Acknowledgments to:
Ivan Viktorov, REAct Project Coordinator in Kyiv Oblast
Svitlana Tkalia, President, Charity Fund “Hope and Trust”, a REActor